|
New approaches are in the pipeline including a 'buprenorphine
implant' that will last 6 months.
WHAT IS DRUG ADDICTION AND WHAT CAUSES IT TO HAPPEN?
Addiction
is a chronic, often relapsing brain disease that causes compulsive
drug seeking and use. Although the initial decision to take
drugs is voluntary for most people, the brain changes that occur
over time challenge a person’s self control and ability to resist
intense impulses urging them to take drugs.
Addiction
affects the brain circuits involved in reward, motivation, memory,
and inhibitory control. When these circuits are disrupted, so
is a person’s capacity to freely choose not to use drugs. In
fact, the inability to stop is the essence of addiction, like
riding in a car with no brakes.
 |
Addiction
is similar to other chronic diseases. PET scans showing
healthy versus diseased brain of a cocaine user and health
versus diseased heart. Using imaging technology to measure
metabolism (in this case, glucose uptake) in the brain
and heart, one can see that both addiction and heart disease
produce observable changes in organ function.
In
each pair of images shown to the left, the healthy organ
shows greater activity (reds and yellows) than the diseased
organ. In drug addiction, the frontal cortex, which is
a part of the brain associated with judgment and decision-making,
is significantly affected. Like heart disease, drug addiction
can be prevented and treated successfully. If left untreated,
however, its effects can last a lifetime.
Image
from
NIDA
|
When drugs
enter the brain, they can interrupt the work and actually change
how the brain performs its jobs. These changes are what lead
to compulsive drug use, the hallmark of addiction.
WHAT
REGIONS OF THE BRAIN DOES DRUG ABUSE AFFECT?
Drugs of
abuse affect three primary areas of the brain: the brain stem,
the limbic system and the cerebral cortex.
|
The
brain stem is in charge of all of the functions our
body needs to stay alive—breathing, circulating blood,
and digesting food. It also links the brain with the spinal
cord, which runs down the back and is responsible for
moving muscles and limbs as well as letting the brain
know what’s happening to the body.
The
limbic system links together a bunch of brain structures
that control our emotional responses, such as feeling
pleasure when we eat chocolate. The good feelings motivate
us to repeat the behavior, which is good because eating
is critical to our lives.
The
cerebral cortex is the mushroom-like outer part
of the brain (the gray matter). Some areas process information
from our senses, enabling us to see, feel, hear, and taste.
The front part of the cortex, known as the frontal cortex
or forebrain, is the thinking center. It powers our ability
to think, plan, solve problems, and make decisions. --Image
source from
NIDA
|
 |
WHAT
HAPPENS IN THE BRAIN?
 |
Normally,
the reward circuit responds to pleasurable experiences
by releasing the neurotransmitter dopamine, which creates
feelings of pleasure, and tells the brain that this is
something important—pay attention and remember it.
Drugs
hijack this system, causing unusually large amounts of
dopamine to flood the system. This flood of dopamine is
what causes the “high” or euphoria associated with drug
abuse.
The
brain adapts in response to the overwhelming surges in
dopamine. The brain adjusts by decreasing the number
of dopamine receptors available– thus diminishing the
function of the reward circuit. Drug addicts are compelled
to abuse drugs to bring their dopamine function back up
to normal, requiring ever larger amounts to achieve the
initial dopamine high– an effect known as tolerance.
Image
and source from
NIDA
|
WHY IS
IT SO DIFFICULT TO HAVE A PERMANENT RECOVERY?
What makes
permanent recovery difficult is that the drug-induced changes
create lasting memories that link the drug to a pleasurable
reward. Since many of the brain circuits that govern learning
and memory are affected by addiction,. long-term memories are
formed by the activity of brain substances (called transcription
factors). So repeatedly taking drugs can change the brain cells
and make the memory of the pleasurable effects very strong.
When a person is addicted, they get conditioned just like Pavlovian
dogs. Even after transcription factor levels return to normal,
addicts may remain hypersensitive and the risk of relapse in
addicts can persist long after they stop taking the drug.
CURRENT
TREATMENTS
Methadone
Methadone
is a synthetic opiate was developed in Germany during WWII because
of a dwindling supply of morphine. Because of its slow metabolic
breakdown, it was later used to block or decrease the cravings
and withdrawal symptoms from persons that were addicted to opiates
such as heroin. Methadone, as an opiate, is a central nervous
system depressant and is not a cure for opiate addiction. Methadone
lessens the cravings for opiates and coupled with counseling,
facilitates recovery. Methadone has a 40-year history of demonstrated
success in the treatment of opiate addiction. When used in proper
doses in maintenance treatment, methadone does not create euphoria,
sedation or an analgesic effect.
Pros
and Cons Weblinks
Methadone
Pros and Cons. Is MMT Right for You?
What
are the pros and cons of treatment with Methadone?
--------------------------------------------
Current
Clinical Trials using Methadone
Buprenorphine
Buprenorphine
is an opioid partial agonist . This means that, although buprenorphine
is an opioid, and thus can produce typical opioid agonist effects
and side effects such as euphoria and respiratory depression,
its maximal effects are less than those of full agonists like
heroin and methadone. At low doses buprenorphine produces sufficient
agonist effect to enable opioid-addicted individuals to discontinue
the misuse of opioids without experiencing withdrawal symptoms.
The agonist effects of buprenorphine increase linearly with
increasing doses of the drug until at moderate doses they reach
a plateau and no longer continue to increase with further increases
in dose—the “ceiling effect.” Thus, buprenorphine carries a
lower risk of abuse, addiction, and side effects compared to
full opioid agonists. In fact, in high doses and under certain
circumstances, buprenorphine can actually block the effects
of full opioid agonists and can precipitate withdrawal symptoms
if administered to an opioid-addicted individual while a full
agonist is in the bloodstream. (source)
Buprenorphine
itself binds more strongly to receptors in the brain than do
other opioids, making it more difficult, regardless of the presence
of the naloxone, to become intoxicated via other opioids when
buprenorphine is in the system. If enough buprenorphine is in
the system, however, it has the same type of effect as naloxone;
i.e., it completely or nearly completely blocks or reverses
opiate effects from other opioids. 0.3 mg of buprenorphine parenterally
is equivalent in antagonistic effect to between 0.4 and 2.0
mg of naloxone parenterally, but with a much longer half-life
(WIKI)
According
to Walter Ling, M.D., Professor of Psychiatry and Director of
the Integrated Substance Abuse Programs (ISAP) at UCLA ..."Buprenorphine
is probably the most important advance in treating opiate addiction
since the introduction of methadone,""The reason is that buprenorphine,
because of its unique pharmacological property, allows the doctors
to be more flexible in its use." "The introduction of buprenorphine
is giving back the treatment of heroin addiction, or all opiate
addiction, to the hands of the physicians.
Buprenorphine
(Suboxone and Subutex) are currently available in pill form
or film form. The pill or film is taken orally to be absorbed
beneath the tongue. Most people take buprenorphine in daily
doses. Many people in early recovery have a hard time holding
and managing their own buprenorphine. Medication is often lost,
stolen or sold.
VIVITROL
Vivitrol
is long-acting form of the opioid antagonist naltrexone. Naltrexone
is used along with counseling and social support to help people
who 'have stopped drinking alcohol and using street drugs' continue
to avoid drinking or using drugs.
The Food
and Drug Administration recently approved Vivitrol for treating
opiate addiction, based on positive research findings in heroin-addicted
patients in Russia. The
study was done with 250 heroin addicts in Russia. It showed
that relapse was reduced (compared to a placebo injection) and
allays narcotic cravings. At the end of six months, 86 percent
of patients taking Vivitrol were drug-free, going to counseling
sessions and functioning in a job or at school, compared to
57 percent of those who got a placebo. (Some experts say that
placebo success rate is higher than they'd expect in this country.)
Naltrexone
should not be started prior to several (typically 7-10) days
of abstinence from opioids. This is due to the risk of acute
opioid withdrawal if naltrexone is taken, as naltrexone will
displace most opioids from their receptors. Naltrexone is only
helpful when it is used as part of an addiction treatment program.
RB'S Suboxone
film
RB’s
Suboxone combines buprenorphine with naloxone,
another drug that deters opioid drug abuse. Suboxone was
first developed as a tablet placed under the tongue. RB
later developed a dissolvable film version, also placed
under the tongue. The product’s sale grew as buprenorphine
continues to grow as an opioid dependence treatment option.
The Suboxone film is the only transmucosal product available.
But Suboxone’s drawback has been an unpleasant taste. Sullivan
said nearly all of his patients complain about the taste,
but they have had no alternative.
IN
THE PIPELINE TREATMENTS
BEMA Buprenorphine
Like Suboxone,
BEMA Buprenorphine combines buprenorphine and naloxone
in a single transmucosal product. BDSI is developing BEMA Buprenorphine
through the U.S. Food and Drug Administration’s 505(b)(2) pathway,
which allows the company to seek approval by showing its product
is bioequivalent to the already-approved Suboxone. A series
of studies requested by the FDA are ongoing or on track to start
in 2012. The last study, a safety study in opioid dependent
patients, is expected to produce data in the first quarter of
2013. BDSI expects it will be in position to file a new drug
application shortly after.
The BEMA
drug delivery technology consists of a small, bioerodible polymer
film for application to the mucosal membranes (inner lining
of cheek). BEMA films are designed to: Adhere to oral mucosa
in less than 5 seconds, optimize delivery across the oral mucosa
and completely dissolve within 15 to 30 minutes. Daily use is
required as with Suboxone.
PROBUPHINE
6 MONTH IMPLANT
Probuphine
is buprenorphine in the form of an implant. The probuphine implant
delivers a constant dose of the drug for six months, eliminating
the need for a daily pill and big obstacle in preventing relapse.
The probuphine implant is a small, solid rod. The implant is
placed under the skin, usually in the upper arm, by a doctor
in a simple office procedure. Probuphine patients get 6 months
of continuous buprenorphine dosing from a single implant. One
of the problems with buprenorphine in pill form is abuse. Doctors
have no way of knowing if their patients are taking the medication
as prescribed or selling the pills to others.
Original
Contribution Buprenorphine Implants for Treatment of Opioid
Dependence: A Randomized Controlled Trial Walter Ling, Paul
Casadonte, George Bigelow, Kyle M. Kampman, Ashwin Patkar, Genie
L. Bailey, Richard N. Rosenthal, Katherine L. Beebe JAMA. 2010;304(14):1576-1583.
read
abstract
In an editorial
accompanying the study, Dr. Patrick O'Connor of the Yale University
School of Medicine, says the study findings represent a potentially
important step forward in treating opiate dependence. "If further
research suggests that this buprenorphine implant is as good
as or better than current treatment approaches," O'Connor writes,
"then the study … would represent a major advance in the substantial
and continued progress that has occurred in the treatment of
opioid dependence since methadone maintenance began in the 1960s."
Subcutaneous
buprenorphine implants (Probuphine™) deliver constant, low levels
of buprenorphine for up to six months with minimal fluctuations
in steady-state plasma concentration, and offer potential treatment
advantages over sublingual buprenorphine by ensuring patient
compliance and limiting diversion. In previous studies, treatment
with buprenorphine implants has been shown to be well-tolerated
and efficacious in significantly reducing illicit opioid use,
retaining patients in treatment, controlling withdrawal symptoms
and opioid cravings, and improving global disease severity.
In recently
released results of a six month, randomized, controlled, phase
3 trial comparing buprenorphine implants to placebo implants
and sublingual buprenorphine/naloxone it was shown that the
implants was non-inferior and comparable to sublingual buprenorphine.
In addition
..."Patients treated with sublingual buprenorphine during
the initial 24 week period and then switched to the probuphine
implants during the 24 week re-treatment phase reported high
levels of satisfaction with the implants in comparison to sublingual
buprenorphine...." see
abstract of data.
Note:
The Probuphine implant is a product of Titan Pharmaceuticals
and is expected to be available in 2013.
Vaccines
against narcotics
The scientists
who are working to create vaccines against narcotics include
Thomas Kosten at the Baylor College of Medicine and S. Michael
Owens at the University of Arkansas and Kim
Janda from Scripps Research Institute. Dr. Kosten has had
limited success with a cocaine
vaccine, while Dr. Owens is focused on vaccines for methamphetamines.
The initial
problem confronting Janda in producing a vaccine was that these
drugs, make terrible targets because they are way too small
for the immune system to even detect them. To overcome that,
Dr. Janda attaches a hapten — which is either a bit of the drug
itself, or a synthetic version of it — to a larger protein that
acts as a platform. The last part of the vaccine is an adjuvant,
a chemical cocktail that attracts the immune system’s notice,
effectively tricking it into making antibodies against a substance
it usually wouldn’t see.
In July
2011 , Janda made news when he announced that an anti-heroin
vax seemed to work in rat experiments (see article in Medical
News Today) meaning it could move into safety trials for
humans. However considering the recent setback with a
nicotine vaccine using a similar approach it appears that
vaccines of this type are still many years away.
|
Drug
Name
|
Molecular
Structure
|
Mechanism
of Action
|
Use
|
|
Buprenorphine
(see
3-D
structure of molecule and information)
|
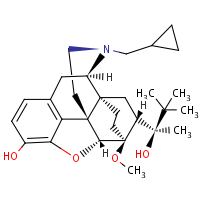 |
Buprenorphine
is a partial opioid agonist. It binds to the µ-opioid
receptors in the brain that are responsible for opioid
intoxication.. Buprenorphine has very high affinity for
µ-opioid receptors receptors and therefore is not displaced
by other opioids. Since it is a partial agonist, it does
not produce as much euphoria but does suppress withdrawal
and cravings.
|
Buprenorphine
is a semi-synthetic opioid that is used to treat opioid
addiction |
|
Naltrexone
(see
3-D
structure of molecule and information)
|
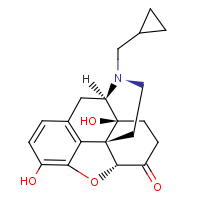 |
Naltrexone
and its active metabolite 6-ß-naltrexol are competitive
antagonists at µ- and k-opioid receptors, and to a lesser
extent at d-opioid receptors |
The
main use of naltrexone is for the treatment of alcohol dependence |
|
Naloxone
(see
3-D
structure of molecule and information)
|
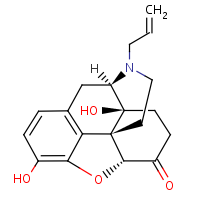 |
Naloxone
appears to antagonize the opioid effects by competing for
the same receptor sites, especially the opioid mu receptor.
Recently, naloxone has been shown to bind all three opioid
receptors (mu, kappa and gamma) but the strongest binding
is to the mu receptor. |
Naloxone
is a drug used to counter the effects of opiate overdose. |
|
Methadone
(see
3-D
structure of molecule and information)
|
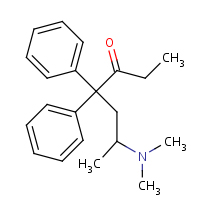 |
Methadone
is a full µ-opioid agonist. Methadone also binds to the
glutamatergic NMDA (N-methyl-D-aspartate) receptor, and
thus acts as a receptor antagonist against glutamate. |
Methadone
is used for treatment of moderate-to-severe pain and maintenance
treatment of addiction to heroin. |
|
Morphine
(see
3-D
structure of molecule and information)
|
 |
Morphine
first acts on the mu-opioid receptors. It has also been
shown that morphine binds to and inhibits GABA inhibitory
interneurons. These interneurons normally inhibit the descending
pain inhibition pathway. So, without the inhibitory signals,
pain modulation can proceed downstream. |
Morphine
is mainly used for treating short-term and long-term pain
in adults |
|
Hydrocodone(Vicodin)
(see
3-D structure of molecule and information)
|
 |
Acts
at µ-opioid receptors |
Vicodin
is used to relieve moderate to severe pain |
|
Oxycodone
--(Ocycontin)
(see
3-D
structure of moleculeand information)
|
 |
The
precise mechanism of the analgesic action is unknown. However,
specific CNS opioid receptors for endogenous compounds with
opioid-like activity have been identified throughout the
brain and spinal cord and are thought to play a role in
the analgesic effects of this drug. |
OxyContin
is used to treat moderate to severe pain |
References
Addiction
Science: From Molecules to Managed Care
Brain
and Addiction
Drug
Implant for Opioid Addiction Looks Effective
Hooked:
Why it's not so easy to "just say no"
Important
Treatment Advances for Addiction to Heroin and other Opiates
--Nora D. Volkow
Drug Abuse.gov
Dopamine
in drug abuse and addiction: results of imaging studies and
treatment implications.
Why
bad habits are hard to break
The
Changing Landscape of Vaccine Development: Vaccines for Chronic
Diseases
An
Addiction Vaccine, Tantalizingly Close
Researcher
Makes a Career Developing Cocaine Vaccine, But Pharmaceutical
Companies Won’t Produce It
Drug
Implant for Opioid Addiction Looks Effective
|