Multiple Sclerosis
Multiple sclerosis (MS) is a demyelinating disease, a non-contagious chronic autoimmune disorder of the central nervous system which can present with a variety of neurological symptoms occurring in attacks or slowly progressing over time. It has no cure yet and the exact cause remains unknown. Due to its effects of the nervous system, it can lead to long-term impaired mobility and disability in severe cases.
History

There are a few early reports about patients who could have suffered from MS. St. Lidwina of Schiedam (1380–1433), a Dutch nun, may have been the first reported MS patient. From the age of 16, she developed intermittent pain, weakness of the legs, and visual loss—symptoms typical of MS. She died at the age of 53.
Augustus Frederick d'Este (1794–1848), an illegitimate grandson of King George III, another famous MS patient, left a detailed diary describing his 22 years living with the disease. It began at 28 with a sudden transient visual loss after the funeral of a friend. During the course of his disease he developed weakness of the legs, clumsiness of the hands, numbness, dizziness, bladder disturbances, and erectile dysfunction. In 1844, he was confined to a wheelchair. Until his death four years later, he kept an optimistic view of life. The British diarist W. N. P. Barbellion also kept a detailed log of his diagnosis and struggle with MS, published in 1919 as The Journal of a Disappointed Man.
Robert Hooper (1773–1835), a British pathologist and practicing physician, Robert Carswell (1793–1857), a British professor of pathology, and Jean Cruveilhier (1791–1873), a French professor of pathologic anatomy, were the first to describe the disease by medical illustrations as well clinical details. Jean-Martin Charcot (1825–1893), a French neurologist, summarised previous reports and made important contributions by his own clinical and pathological observations. He recognised multiple sclerosis (sclerose en plaques) as a distinct, separate disease.
After 130 years of intensive research, we now know much about the underlying factors surrounding MS, and effective treatments have been developed. MS, however, is still an incurable disease, and the fundamental causes are unknown.
Prevalence
In northern Europe, continental North America, and Australasia, about one of every 1000 citizens suffers from multiple sclerosis, whereas in the Arabian peninsula, Asia, and continental South America, the frequency is much lower. In Sub-Saharan Africa, MS is extremely rare. With important exceptions, there is a North-South gradient in the Northern hemisphere and a South-North gradient in the Southern hemisphere, with very low frequencies near the equator. Climate, diet, geomagnetism, toxins, sunlight, genetic factors, and infectious diseases have been discussed as possible reasons for these regional differences. It has been postulated that an environmental factor during childhood might play an important role for the development of MS later in life. This was based on several studies in migrants demonstrating that if migration occurs before the age of 15, the migrant acquires his new region's susceptibility to MS. If migration takes place after 15, the migrant keeps the susceptibility of his home country.
MS occurs mainly in the Caucasian race. It is 20-fold lower in the Inuit people of Canada than in other Canadians living in the same region. It is also rare in the Native American tribes of North America, the Australian Aborigine and the Maori of New Zealand. These few examples point out that the genetic background plays an important role in the development of MS (see below).
As observed in many autoimmune disorders, MS is more common in females than males; the mean sex ratio is about two females for every male. In children, who rarely develop MS, the sex ratio may reach three females for each male, whereas MS occurring in the fifth decade more commonly affects males. Onset of symptoms usually occurs between 20 to 40 years of age, rarely below 15 or above 60, although both are possible.
MS is not strictly a hereditary disease. However, MS is a disease influenced by a variety of factors, one of which is the genetic background of an individual. There is no single gene known to be responsible for MS, though a few genes have been demonstrated to increase the risk of development. Although these genes are of scientific interest and continue to play a part in research, they are not enough to diagnose an individual with MS.
Overall, on average one of every 25 siblings of an individual with MS will also be afflicted. Up to every second identical twin of a MS-affected person will develop MS, but only one of 20 fraternal twins. If one parent is affected by MS, each child has a risk of only about 1 in 40 to develop MS later in life.
Cause
The ultimate cause of MS is unknown. It is hypothesised that a viral infection or other environmental factor in childhood might prime the immune system for an abnormal reaction later in life. On a molecular level, there might be a structural similarity between an unidentified infectious agent and components of the central nervous system, causing confusion in the immune system later in life (a process called "molecular mimicry"). However, so far there is no known "MS virus". Certainly MS is not contagious. The importance of genetic factors has been discussed above.
It is widely accepted that a special subset of white blood cells, called T cells, play a key role in the development of MS. Under normal circumstances, these lymphocytes can distinguish between self and non-self. In a person with MS, however, these cells recognize healthy parts of the central nervous system as foreign, and attack them as they would a virus. In MS, the part of the nervous system primarily attacked is myelin. Myelin is a fatty substance that covers the axons of nerve cells, and which is important for proper nerve conduction. Normally, there is a tight barrier between blood and brain, called the blood-brain barrier (BBB), built up of endothelial cells lining the blood vessel walls.
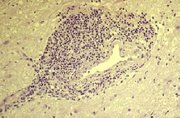
In MS, the BBB breaks down; autoreactive T cells cross the BBB and trigger an inflammatory process, also mediated by other immune cells and soluble factors, such as cytokines and antibodies. Due to this abnormal behavior of the immune system, MS is considered to be an autoimmune disorder. The inflammatory process finally leads to opening of the BBB; this can cause a number of factors, such as edema, upregulation of adhesion molecules on endothelial cells. This also causes activation of macrophages, activation of MMPs, other proteases and cytokines. This will lead to a destruction of myelin, called demyelination.
Repair processes, called remyelination, also play an important role. This is one of the reasons why, especially in early phases of the disease, symptoms tend to decrease or disappear temporarily after days to months. Nevertheless, axonal damage and irreversible loss of neurons occur early during the course of the disease. However, due to its plasticity the brain can often compensate for some portion of the damage. MS symptoms develop as a result of multiple lesions in the brain and spinal cord, and can vary greatly between different individuals, depending on where the lesions occur.
The original oligodendrocytes that form the myelin sheath are incapable of re-creating the sheath once it has been destroyed. However, the brain is capable of recruiting progenitor cells, which migrate from other unknown regions of the brain, differentiate into mature oligodendrocytes, and re-make the myelin sheath. This new myelin sheath is often not as large or effective as the original, though, and repeated attacks will have successively less effective remyelinations, until a plaque is built up around the damaged axons. Progenitor cells are very capable of differentiating and remyelinating axons in vitro; it is therefore suspected that inflammatory conditions and/or axonal damage inhibit progenitor cell differentiation in vivo.
Diagnosis
A definite diagnosis of MS requires evidence for dissemination of lesions within the central nervous system both in space and in time. This means that not only must there exist evidence of at least two distinct lesions, verifiable by clinical symptoms or by Magnetic Resonance Imaging (MRI), there must also be evidence of an occurrence of new symptoms or lesions within a time interval of at least 30 days. A lumbar puncture, which is a procedure done to collect a sample of cerebrospinal fluid, is useful for providing evidence of chronic inflammation of the central nervous system, often indicated by oligoclonal banding. Nerve conduction studies of optic, sensory and motor nerves can provide further evidence for MS, as the process of demyelination results in reduced nerve conduction velocities. The diagnostic process is completed by several laboratory tests to exclude other diseases that can mimic MS, such as sarcoidosis, vasculitis, and Lyme disease.
Signs and symptoms
Affected individuals may experience a wide variety of symptoms, such as vision loss, double vision, nystagmus, difficulty with speech, various kinds of tremor, clumsiness of the hands, unsteady gait, weakness, spasticity, numbness, and bladder, bowel, as well as sexual dysfunction. Various cognitive impairments are also common, such as difficulty performing multiple tasks at once, difficulty following detailed instructions, loss of short term memory, depression, and fatigue.
Disease course and clinical subtypes
In most cases MS starts with an acute flare-up of symptoms within hours to days, called a relapse, exacerbation, bout, episode, or attack. Inflammation of an optic nerve (optic neuritis), causing painfulness of eye movement and visual deterioration frequently is the first symptom. However, not all patients with optic neuritis develop MS. Sensory disturbances such as numbness or tingling sensations are other frequent initial symptoms. In principle, MS can start with any of the symptoms mentioned in the section above.
Especially in early phases of the disease, symptoms frequently decrease or resolve spontaneously within days to months. Therefore, this disease course is called relapsing remitting. New relapses can occur within weeks to many years and can include formerly experienced and/or new symptoms. However, MRI studies have shown that nerve damage can continue in relapsing remitting patients even if symptoms subside. It has long been known that "MS never sleeps". This highlights the importance of preventive treatment if and when it is available.
In many cases, the disease course changes after several years and symptoms start to deteriorate slowly with or without superimposed relapses. This course is called secondary chronic-progressive, or just secondary progressive. However, some patients stay in a relapsing remitting course for the rest of their lives.
About 10% of all MS-affected individuals experience chronic progression without relapses from onset of symptoms. This course is called primary progressive and frequently comes along with weakness of the legs, gait and bladder disturbances. Degenerative processes and not inflammation are thought to play the most important role in this clinical disease course.
Chronic progression from onset of symptoms with superimposed relapses is referred to as relapsing progressive.
Factors triggering a relapse
In general, relapses tend to occur more frequently during spring and summer than during autumn and winter. Infections like the common cold, influenza or unspecific diarrhea increase the risk for a relapse. In contrast, influenza vaccination is safe and does not trigger relapses as demonstrated in several recent studies. It can therefore be recommended for MS patients, especially for those at risk for influenza (e.g. healthcare workers). Tetanus vaccination is considered to be safe as well, although so far it has not been studied in that detail. In general, vaccinations with living, attenuated viruses increase the risk of relapses.
Pregnancy can directly affect the susceptibility for relapse. The last three months of pregnancy offers a natural protection against relapses, whereas during the first few months after pregnancy, especially during the first six weeks, the risk for a relapse is increased 20-40%. According to current knowledge, pregnancy doesn't seem to influence long term disability. MS does not increase the risk of bearing a handicapped child.
Statistically, there is no good evidence for triggering of relapses through trauma or operations. In principle, surgical procedures require no special precautions if not dictated by existing disability. Participation in sports is possible, although extremes, such as marathon running, should probably be avoided. Emotional stress may cause a relapse, although study data has been inconsistent.
Heat can transiently increase symptoms, in something known as Uhthoff's phenomenon. This is why some patients avoid saunas or even hot showers. However, heat is not an established trigger of relapses. Extensive exposure to the sun should be avoided, since ultraviolet radiation is a strong stimulus for the immune system.
Prognosis
Because of improved treatment for complications such as lung and bladder infections, the life expectancy of those diagnosed with MS is only slightly reduced. The earlier in life disease onset occurs, the slower disability progresses. This is due to more frequent chronic progressive courses with faster accumulation of disability when onset occurs at a higher age. Disability after 5 years correlates well with disability after 15 years: 2/3 of MS patients with low disability after 5 years will not markedly deteriorate during the next ten years. Further MS cases in the family do not influence disease progression. 1 of 3 patients will still be able to work after 15-20 years. Visual loss as the initial symptom is a marker for a rather good prognosis; gait disturbance, weakness or numbness for a rather poor prognosis. Rapid regression of initial symptoms, age at onset below 35, only a single symptom at onset, rapid development of initial symptoms and short duration of the last relapse indicate a good prognosis. When the initial disease course is relapsing remitting, the statistical duration until a wheelchair is needed, is 20 years. This means that many MS patients will never need a wheelchair. If the disease course is primary progressive then a wheelchair at an average will be needed after 6 to 7 years. It has to be noted that most of this longterm data was acquired before the advent of modern immunomodulatory drugs about 10 years ago, which have been shown to delay disease progression over a period of several years.
Currently there are no clinically established laboratory investigations available to predict prognosis or therapeutic response, although promising approaches have been undertaken that need further confirmation, such as determination of the two antibodies anti-MOG and anti-MBP or of TRAIL (TNF-Related Apoptosis Inducing Ligand).
Treatment
There is no known definitive cure for multiple sclerosis. However, several drugs have proven to be effective in its treatment. Intensive research is underway to study a variety of promising new drugs. Treatment is aimed at maintaining a maximum quality of life. Physiotherapy plays an important role.
There are three primary forms of medication used to treat the symptoms:
- During an exacerbation, corticosteroids (such as prednisone or methylprednisolone) used at high dosages (500 mg–2 g per day intravenously for a course of 3 to 5 days) can accelerate regression of symptoms. Subsequent tapering with pills may be reasonable in certain cases. There is clear evidence that sole treatment with oral steroids at dosages of 100 mg per day or less and subsequent tapering is inferior to intravenous high dose treatment. In principle, steroid treatment during pregnancy is possible. There is no good evidence that corticosteroids influence longterm outcome.
- Long-term
treatment can influence the course of the disease:
- Interferon-beta1a or beta1b (Avonex; Betaseron [in Europe Betaferon]; Rebif) has been shown to reduce the relapse rate by about 30%, decrease the number of new MRI lesions and slow progression of disability. Interferon-beta is a cytokine that under natural conditions is produced by the body during viral infections; as a drug it is extracted either from special mammalian cells or special bacteria. All preparations must be injected into either muscle or skin every second day to once per week, depending on the preparation. Attempts to develop pills containing Interferon-beta have not been successful so far. Some of the interferons have been proven to be effective not only in relapsing remitting MS, but also in secondary progressive MS, as long as superimposed relapses occur. Main side effects include flu-like symptoms which tend to decrease during ongoing therapy and which can be alleviated, for example, by paracetamol or ibuprofen. Another frequent side effect is inflammatory skin reactions at the injection site if Intereferon-beta is injected into the skin. Regular blood monitoring is required.
- Glatiramer acetate (Copaxone) has also been shown to reduce the relapse rate by about 30%, decrease the number of new MRI lesions and slow progression of disability. Concerning its therapeutic effect it is approximately comparable to Interferon-beta. Glatiramer acetate consists of synthetic peptides made of four different amino acids, which are basic modules of all proteins in the human body. Once per day must be injected into the skin. Attempts to develop pills containing glatiramer acetate have also been unsuccessful. Copaxone is effective in the treatment of relapsing remitting MS. So far, beneficial effects in secondary progressive MS have not been convincingly demonstrated. Main side effects include inflammatory skin reactions at the injection site, and a rare but transient and perturbing "post-injection" reaction manifested by flushing, chest tightness, heart palpitations, breathlessness, and anxiety. A post-injection reaction does not require discontinuation of therapy. In general, Copaxone is considered to cause fewer side effects than Interferon-beta. However, most MS patients injecting Interferon-beta also tolerate their therapy well. Regular blood monitoring is required.
- Azathioprine is an agent available as a pill approved for the treatment of relapsing remitting MS in some countries. However, its effectiveness has not been proven as stringently as for the interferons and glatiramer acetate, and an effect in secondary progressive MS has not been demonstrated. In general, it is well tolerated. After longtime therapy the risk of cancer increases slightly (after 10 years of therapy about fourfold). Regular blood monitoring is required.
- There is some evidence that immunoglobulins (antibodies) are effective in the treatment of relapsing remitting MS, a large clinical trial (PRIVIG) is presently continuing. Immunoglobulins have not been proven to be effective in secondary progressive MS.
- The currently most effective drug in the preventive treatment of MS is Mitoxantrone. It has been proven to be effective in relapsing remitting and in secondary progressive MS. In most cases it is administered every three months intravenously. Therapy with Mitoxantrone is generally well tolerated, however, since with ongoing therapy the risk for damage of the heart muscle increases, at an average Mitoxantrone can only be administered for 3 to 4 years. This is why Mitoxantrone is only used in cases of rapid disease progression. Mitoxantrone treatment requires monitoring of the heart function during therapy. Regular blood monitoring is required. With these precautions Mitoxantrone treatment is safe.
- Several other immunosuppressive drugs, such as cyclophosphamide (Cytoxin) or methotrexate, may be helpful in some cases. Efficacy of these drugs has not been proven very stringently.
- A family of cholesterol-lowering drugs, the statins, have shown anti-inflammatory effects in animal models of MS. However, so far there has not been provided sufficient evidence that statins are beneficial in the treatment of human MS patients with normal cholesterol levels.
- A recent study found that women who took vitamin D supplements were 40% less likely to develop multiple sclerosis than women who did not take supplements. However, this study does not allow to conclude that vitamin D has a beneficial influence on ongoing MS. Furthermore it could not distinguish between a beneficial effect of vitamin D and multivitamin drugs including vitamin E and various B vitamins which may also exert a protective effect.
- Primary progressive MS is very difficult to treat. High dose corticosteroids every three months can show some effect. In principle, there is no efficient preventive treatment for primary progressive MS available. Symptomatic therapy as described in the next paragraph and physiotherapy play an important role.
- A variety of medications
are used to treat symptoms without influencing the inflammatory nature of the
disease (symptomatic treatment):
- Baclofen and tizanidine can be useful against spasticity. There is no convincing evidence that cannabinoids (marijuana) can improve spasticity.
- The anticonvulsant drugs Gabapentin and Carbamazepine and the antidepressant amitriptyline can improve pain and tingling sensations in certain cases.
- SSRIs be used for depression, as well as for fatigue. Fatigue can also be influenced by amantadine and modafinil.
- There is also treatment for bladder disturbances available which is effective in many cases. Examples are oxybutynin and trospium chloride.
- Treatment with sildenafil (Viagra®) or similar substances can improve male erectile dysfunction in many cases.
Additional treatment options include plasmapheresis ("washing the blood", showing similarities to dialysis) for severe, non-steroid responsive relapses.
External links
- National Multiple Sclerosis Society (http://www.nmss.org)
- Multiple Sclerosis Society (http://www.mssociety.org.uk)
- Multiple Sclerosis Society of Canada (http://www.mssociety.ca)
- Multiple Sclerosis Society of Germany (http://www.dmsg.de)